Case Competition 2023 Case 19 Pushing the Limits of Lower Extremity Reconstruction
Authors: Oliver Didzun, MD, Ludwigshafen, Germany
A 66-year old male patient with bilateral genu varum deformity underwent a valgus-producing lateral tibial head osteotomy with angle-stable plate osteosynthesis and fibular resection osteotomy. During this procedure, iatrogenic injury to the left popliteal artery and vein occurred. Vascular reconstruction was performed the following day using a bovine patch plastic, as well as arterial and venous microsurgical end-to-end anastomosis of the injured vessels. During revision surgery, a complete compartment release of the left lower leg was necessary. Subsequent sequelae included injury to the common peroneal nerve and tibial nerve, along with significant rhabdomyolysis and necrosis of the anterior muscle compartment. Therefore, radical necrosectomy was performed, resulting in a 35 x 4 cm soft-tissue defect on the ventral and a 35 x 5 cm soft-tissue defect on the dorsal aspect of the left lower leg. The patient was then transferred to our tertiary care hospital for specialized defect reconstruction. The patient’s medical history was remarkable for left bundle branch block, arterial hypertension, and non-insulin-dependent diabetes mellitus.


Before and after
Patient examination
Upon admission to our hospital, on assessment, the 66-year-old male patient was in good general health with a slim nutritional status. On the ventral aspect of the left lower leg, there was a 35x4cm soft-tissue defect, with an exposed plate osteosynthesis proximally and exposed tibia longitudinally up to the middle aspect of the lower leg. On the dorsal side, there was a 35x5cm soft-tissue defect with exposed musculature. Dorsally, unlike ventrally, all functional structures—including tendon components, nerves, and vessels—were completely covered with vital musculature. Intact skin bridges were also noted between the soft-tissue defects, indicating that they did not communicate with each other. Blood tests on admission showed a blood glucose level and HbA1c value within the normal range. An angiography was performed, revealing a regular three-vessel supply to the affected lower left leg.
Pre-Operative Considerations
Reconstructive surgery faces a significant challenge when addressing complex and extensive soft tissue loss in the lower extremity. Use of combined free flaps offers a promising strategy for one-stage reconstruction of such defects. The following preoperative considerations were taken into account: 1. A soft-tissue defect measuring 35x4cm was present on the ventral side of the lower left leg. In the proximal section of the defect, there was exposed plate osteosynthesis and tibia. In the distal portion of the defect, the functional structures such as tendons and bones were not exposed. 2. Considering the configuration of the soft-tissue defect and the patient’s high functional demand due to dependency on orthotic support (peroneal splint), the utilization of a split-thickness skin graft in the distal portion of the ventral defect was rendered possible but inadequate to fulfil the functional requirements. Consequently, the decision was made to proceed with full-thickness tissue replacement using a free autologous flap. 3. Based on the potential need for future bone revision procedures, such as removal of the osteosynthesis plates and screws, use of a fasciocutaneous flap was preferred over a muscle flap (e.g., latissimus dorsi free flap) for defect reconstruction. 4. Upon assessment of all available options, and taking into account the patient’s slim nutritional status, we considered that a viable option would have been to use an extended anterolateral thigh (ALT) free flap reaching up to 35 cm in length. However, preoperative perforator mapping using Duplex ultrasonography identified insufficient distal ALT perforators. 5. Another option identified during pre-operative planning was the use of a bilateral ALT-flap up to 35 cm in length. At this stage a decision was made to intraoperatively check for distal ALT-perforators and change to bilateral ALT-flap if perforators were found to be insufficient. During surgery, a third, and more promising option, arose. Although there were insufficient distal ALT perforators, a significant anteromedial thigh (AMT) perforator was available. To circumvent the aforementioned perfusion challenge associated with the unilateral ALT flap, we ultimately opted to perform a combined ALT and AMT free flap, allowing for primary closure of the donor-site. This option not only allowed complete defect reconstruction, but also simultaneously guaranteed adequate perfusion, thus, reducing donor-site morbidity. For the more superficial dorsal defect, split-thickness skin grafting was performed. The patient was provided with detailed information regarding the surgical procedure, which included a clear explanation of the potential risks associated with free flap surgery. These risks included the possibility of partial or total flap loss, as well as complications at the donor-site, such as seroma, hematoma, dehiscence, and loss of strength. The importance of close monitoring of the flap during the initial post-operative to quickly detect and address any potential complications was also explained. Specifically, according to our hospital’s protocol, flaps are monitored hourly during the first 48 hours after the surgery. Furthermore, the possibility of modification of the initially planned procedure intra-operatively if a better option becomes available was also explained.

Step 1: Wound bed preparation
The wound bed was prepared by debriding non-viable tissue and taking precise measurements of the skin and soft tissue defect. Exposed functional structures were identified and measured. A 9 cm segment of exposed plate osteosynthesis and an 18 cm segment of exposed tibia were visible.

Step 2: Flap dissection
At the beginning of the surgical procedure, the borders of a significant Anterolateral Thigh (ALT) flap were delineated and demarcated on the donor site at the right thigh, using a sterile marker. During the operation, the distal ALT perforators were found to be inadequate for the intended purpose. However, an adequate AMT perforator was identified. As a result, a conjoined ALT and AMT flap was selected as the preferred option. The flaps were designed in a manner that enabled closure of the donor site.

Step 3: Flap Assessment
This was followed by preparation of both flaps, each with an independent vascular supply, with simultaneous preparation of the recipient-sites by a second surgical team. By utilizing distinct vascular supplies for each flap, the rectus femoris muscle’s integrity was preserved, resulting in decreased discomfort for the patient and faster recovery.

Step 4: Modelling
The flaps were accurately modeled to meet the defect configuration and two Charrier Redon drains were inserted.
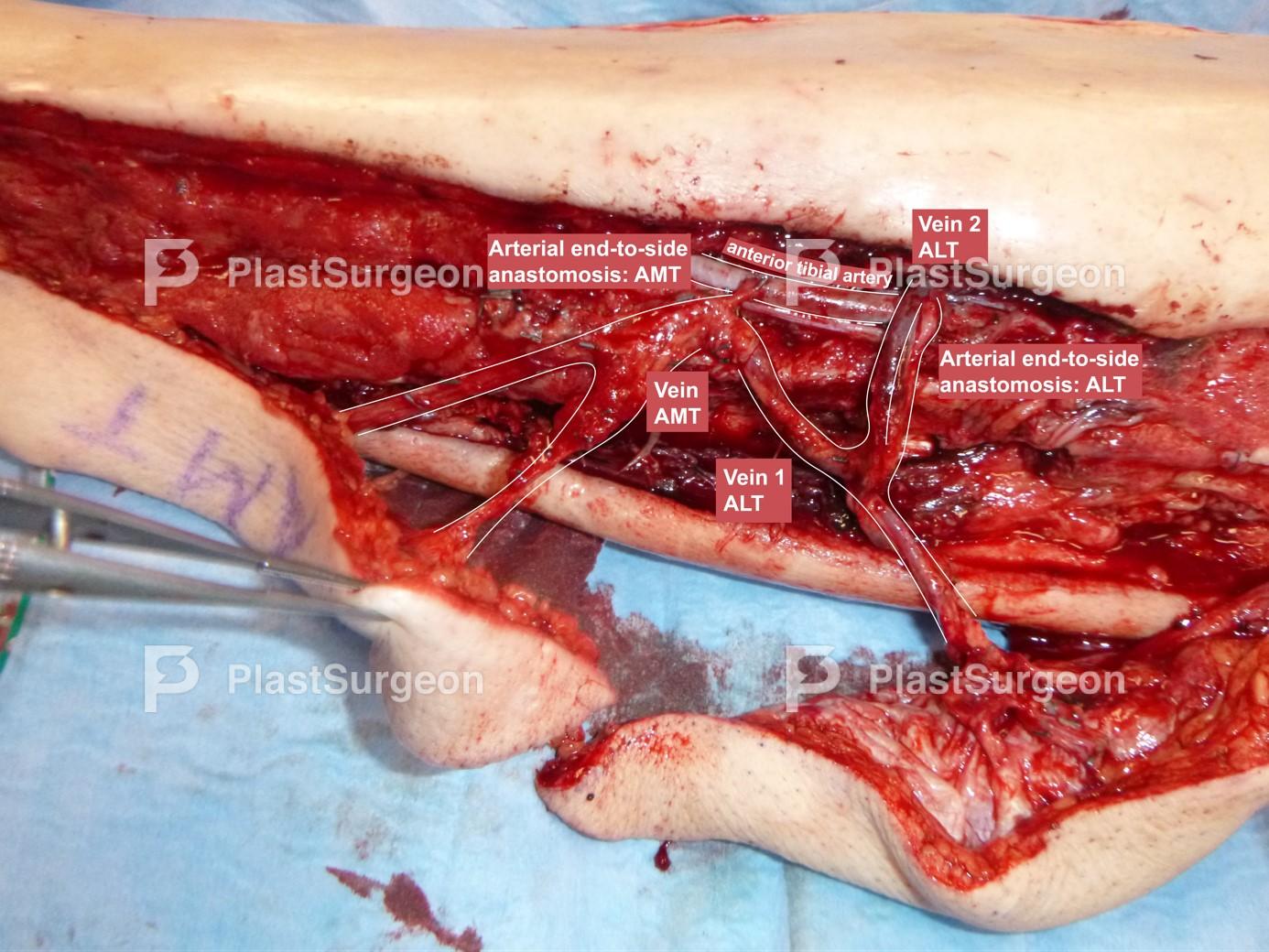
Step 5: Microsurgical anastomoses
Microsurgical anastomoses of the perforators of the two flaps: arterial anastomoses to the anterior tibial artery were established in an end-to-side fashion. The veins were anastomosed to the concomitant veins of the anterior tibial artery and a superficial vein using a venous coupler.

Step 6: Securing
Securing of the flaps through a self-resorbing subcutaneous and intracutaneous suture.

Step 7: Follow-up 12 months – Donor site
The donor site has healed adequately, with no signs of complications or any evidence of wound healing complications or disturbances. At the 12-month follow-up, the patient has been able to resume daily activities without any limitations.

Step 8: Follow-up 12 months – Healing of flaps
The flaps healed completely without evidence of wound healing disorders or flap necrosis. Additionally, the exposed tibia and plate osteosynthesis have been appropriately covered, allowing the patient to safely undergo physiotherapy and use a peroneal splint without restrictions.

Step 9: Follow-up 12 months – Healing of flaps
The flaps healed completely without evidence of wound healing disorders or flap necrosis. Additionally, the exposed tibia and plate osteosynthesis have been appropriately covered, allowing the patient to safely undergo physiotherapy and use a peroneal splint without restrictions.
Post-Operative Plan
– The patient should remain sedentary in bed for five days with hourly monitoring of the perfusion of the flaps by the surgeon for 48 hours. – Following that, the flaps undergo flap dangling to gradually subject the flaps to the increased venous pressure induced by the gravitational forces. – The patient must be monitored on an outpatient basis and scheduled for follow-up visits at two weeks, six weeks, three months, and 12 months after the surgery.
- Achievement of a favourable aesthetic and functional outcome with low risk of re-exposure of the bone, even under the high functional load associated with the use of a peroneal splint.
- Minimal morbidity of the donor-site due to preservation of the rectus femoris muscle and successful primary wound closure.
- Pre-operative planning can be discounted intra-operatively when a more viable option becomes evident. This highlights the importance of adequately consenting patients of this possibility.
- Simultaneous use of two independent free flaps for soft-tissue defect reconstruction is ambitious and requires significant microsurgical experience on the part of the involved surgeons.
- Extended surgery time due to the use of two separate free flaps.
- Performing a minimum of four microsurgical anastomoses is required, which increases the risk of microvascular complications.
References
- Abbassi O, Freer F, Sing QQY, Hoshimatsu H, Karakawa R, Song D, Pafitanis G. Multi-pedicled long fasciocutaneous free flaps in complex lower extremity reconstruction. J Plast Reconstr Aesthet Surg. 2022 Feb;75(2):893-939. doi: 10.1016/j.bjps.2021.11.097. Epub 2021 Dec 1. PMID: 34896041.
- Jia YC, Chen HH, Kang QL, Chai YM. Combined Anterolateral Thigh and Anteromedial Thigh Flap for Extensive Extremity Reconstruction: Vascular Anatomy and Clinical Application. J Reconstr Microsurg. 2015 Nov;31(9):674-80. doi: 10.1055/s-0035-1558985. Epub 2015 Aug 10. PMID: 26258916.






































