Preoperative assessment
Authors: Mia Demant, MD, Christian Kaare Paaskesen med. student, Hasan Gökcer Tekin, MD, Magnus Balslev Avnstorp, MD and Mia Steffensen, MD
Indications for endocrinologic and surgical assessment
No indications for assessment:
- Lower grades of GM/pseudo-GM (Tanner scale 1-2)
Indications for endocrinologic assessment:
- Pronounced discomfort
- Persistent GM (more than a year)
Indications for plastic surgery (1):
- Tanner Scale 3-5 (see above),
- BMI ≤ 25 kg/m2, and
- Unbearable tenderness and social embarrassment
- Normal hormonal status
- Non-smoker
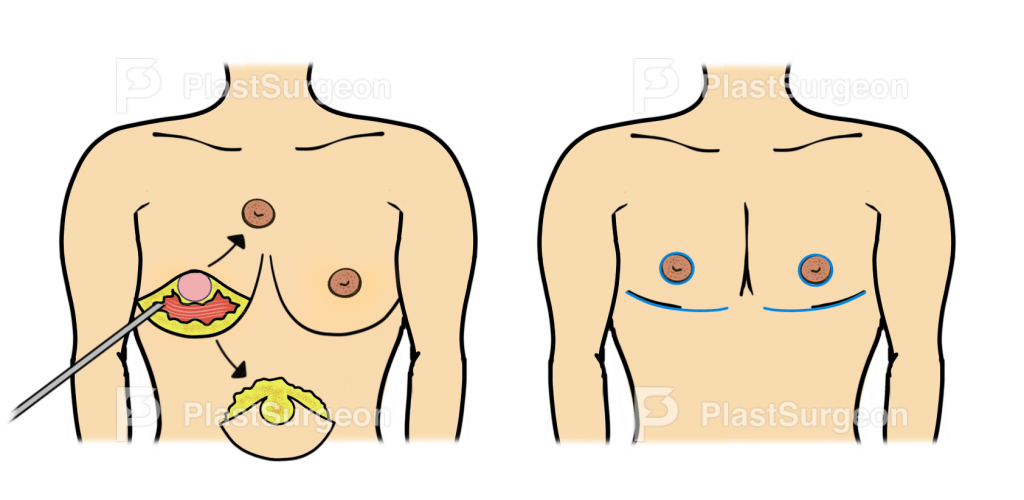
Choosing appropriate surgical technique
The surgical technique depends on the size of the breast, skin elasticity and the skin envelope/residual skin (2). Different surgical approaches can be used depending on the patient’s anatomy (3):

Depending on the chosen technique, certain risks must be taken into consideration:
Semicircular incision
- Less visible scar
- Higher risk of hematoma
- Chest discrepancy because of remaining tissue in the upper chest

Periareolar approach
- Scaring around the NAC

Subcutaneous mastectomy
- Wide and distinct scar
Preoperative information
Pre-operative expectation alignment is essential, and information includes the risk of bleeding, seroma, loss of sensation, scarring, indented nipple and necrosis of nipple and skin.
Postoperative care
Vitality of NAC is controlled with capillary response. Compression garments has to be worn for 2-4 weeks. No lifting of more than 5 kilograms and no sports/physical activities for 3-4 weeks after surgery.
Follow-up
Clinical control 3 months after surgery.
Pearls and pitfalls
- Leave significantly more tissue under the NAC so that this will not fall inwards
- Use a purse-suture to define the desired NAC diameter
- To allow maximum skin retraction, consider a minimal-scarring technique (liposuction or semicircular) following a second stage procedure after 6 to 9 months
- Be careful with under/over-resection when performing liposuction alone
- Drug-induced gynecomastia takes several months to recover from
Acknowledgments
Illustrators: Christian Paaskesen, med.stud.
References
- Paulsen JF, Berg JO, Kroman N, Mieritz M, Jørgensen N. [Gynaecomastia]. Ugeskr Laeger. 2018 22;180(4).
- Thorne, Charles Hm et al, Grabb and Smith’s Plastic Surgery (Wolters Kluwer, 7th ed, 2013;2014;)
- Rohrich RJ, Ha RY, Kenkel JM, Adams WP Jr. Classification and management of gynecomastia: defining the role of ultrasound-assisted liposuction. Plast Reconstr Surg. 2003 Feb;111(2):909-23; discussion 924-5. doi: 10.1097/01.PRS.0000042146.40379.25. PMID: 12560721.





















